Conventional orthodontic treatment recommended extraction of four healthy bicuspid teeth for a 12-year-old, Melissa T. to make room for the crowded remaining teeth. The crowding was created by under development of the patient's dental arches. By removing teeth the genetic potential for growth of the patient's jaws would be compromised. When teeth are extracted and then the upper front six anteriors are retracted, the skull becomes jammed. Since the sutures, spaces between the skull bones, are viable structures (nerves, blood vessels and fibers) the contents become compressed creating neurologic (potential for chronic pain) and structural problems (scoliosis, disc compression and herniation).
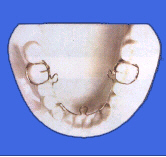
A viable alternative is the use of ALF (Alternative Lightwire) appliances. Since there is no bulky plastic there is no speech problem. It is easy to clean. The patient does not remove it. The forces generated are light therefore reducing pain. The concept is very simple: with light gentle forces, the skull bones will expand and growth stimulated. With increased jaw space there is now room to guide the crowed teeth into a corrected position with conventional orthodontic braces. The other major key is that the ALF appliance must be adjusted at each visit to realign the skull bones. By so doing the foundation of the skull (maxillae- upper dental arch) is leveled. This leveling is important in reducing the amount of relapsing of the teeth into their old crooked position. Balancing the skull bones helps insure a more normal neurologic and spinal function through out the patient's life.
|
||
|
||
|






It is not often a major breakthrough occurs in our professional lifetime that has a monumental impact on patient treatment. The ALF appliance represents just such a discovery. Thanks to the genius and perseverance of Dr. Darick Nordstrom and laboratory technician Heather Ashton the ALF appliances are custom designed to help correct cranial base and cranial distortions present in the chronic pain, orthopedic/orthodontic type patient.
Dental orthopedics and orthodontic programs focus primarily on aligning the teeth and jaw misalignments. The fact remains that cranial lesions and the cranial base must first be corrected inorder to establish long term stability to the stomatognathic system, spine and pelvis. As Major DeJarnette, founder of the SOT chiropractic concept, stated " the anvil (maxillae) must be balanced inorder for the hammer (mandible) and TMJ's to function properly." Other than elongating a pre-maxilla or widening a narrowed maxillae or disimpacting a retruded maxillae with reverse headgear little if any treatment is directed toward correcting transverse or sagittal cants of the maxillae, a torsioned maxillae, high sphenoid, side bending or rotation lesions of the sphenobasilar symphysis. Addressing these cranial issues are critical to resolving the patient's neurophysiologic symptoms and structural imbalances.
Diagnosing abnormal cants of the maxillae is now easily accomplished by means of an invaluable diagnostic instrument, the Accu-Liner articulator. This device provides an accurate, reproducible assessment of the position of the maxillae in relation to Camper's Plane (Hamular Notch/Incisive Papilla Plane). This instrument provides an invaluable tool in orthopedic/orthodontic analyses. Complementary data will also include cephalometric analysis and cranial evaluation: an assessment of the sphenobasilar junction, side bending and/or rotational lesions, torsions and internal and external temporal bone rotations. This data provides a structural configuration of the distortions and provides the basis for designing the ALF appliances. Designing appliances just to correct teeth when cranial base and other distortions exist is really treating the symptom rather than the underlying cause.
The physiologic action of the ALF appliance is consistent with the Arndt-Schulz Law: "Weak stimuli increase physiological activity and very strong stimuli inhibit or abolish activity." The light .025to .028 Elgiloy body wire provides the needed flexibility to allow the cranium to unfold during treatment. The following are additional advantages:
- ALF appliances are much easier to adjust and do not require the expertise
- ALF provides excellent development of the intercuspid area while also
- ALF functions as a continuous unit from molar clasp to molar clasp making the
- ALF is easily inserted without the need to place spacers two days before
- ALF provides constant light forces for more effective cranial movement.
- ALF appliances do not hamper speech, are totally esthetic, can easily be worn
- ALF is a universal treatment system that is custom designed to meet each
- ALF is powerful enough to make rapid corrections yet unobtrusive to allow long-term function necessary for true bony changes.
- Auxiliary wires can be soldered on during later stages of treatment to meet specific needs. Such examples are: elastic hooks, Hawley bow, arms to distalize molars, anterior or posterior acrylic bite planes, fingersprings, lip bumper, buccal tubes to tie into a conventional bracket system, Class III arms for either elastics or reverse pull headgear, twin block acrylic pads and others.
Case Study
A 16 year-old male hit the left side of his head on a basketball pole while going up for a shot. Eventhough the pole was padded the impact was sufficient to cause a concussion and the patient was knocked unconscious for 3 minutes. As a result of the head trauma, the patient suffered severe left sided symptoms: constant headaches, retrobulbar eye pain, tinnitis, facial pain in the region of the cheek, shooting neck and shoulder pain. The patient also had hyperacusis, insomnia and dizziness. Extensive medical work ups by neurologists, ENT, internists and psychiatrists produced no definitive diagnosis. Various medications were prescribed with no resolution of symptoms. These symptoms were present for a seven month period and prevented the patient from attending school.
Cranial Evaluation
The impact had caused a reversal of sphenobasilar motion, decreased amplitude on the left side of the cranium, left internal rotation of the temporal and malar bones, high right sphenoid with torsion in relationship to the occiput.
Dental Evaluation
A mild Class III skeletal discrepancy was present with a mild right posterior crossbite. This malocclusion existed prior to the incident but was accompanied without any symptoms. Extensive spasms were present in the following muscles: right and left external pterygoids, left masseter at the zygoma, right and left anterior temporalis, left scalenes and left upper trapezius.
Treatment Sequencing
- Cranial manipulation was performed to correct the reversed sphenobasilar motion, free up the left temporal and malar and increase amplitude.
- Micro-current stimulation combined with myofascial release techniques were used to release the spastic muscles.
- ALF upper and lower appliances to correct cranial distortions.
- Glutathione was used to detoxify the patient's liver from all the medications that were used.
References
- Frymann,Viola M.: Cranial Osteopathy and Its Role in Disorders of the Temporomandibular Joint. Dental Clinics of North America, W.B. Saunders, Vol. 27, No.3, pp.595-611, 1983.
- DeJarnette, Major B.: Cranial Technique 1979-1980, p.23.
Prognosis: Excellent
The hyperacusis resolved and the headaches greatly reduced following the third cranial adjustment. Following two months of treatment with ALF appliances the cervical and shoulder symptoms and insomnia cleared.The appliances were discontinued following resolution of symptoms.
Use of the ALF appliances affords the dentist a means to non-invasively correct structural distortions which in turn have the potential to cause neurologic and physiologic changes throughout the body. No other medical specialty has the modalities to make these types of changes. Use of the ALF appliance complements the osteopath, chiropractor, physical therapist, psychiatrist, orthopedist and neurologist as well as the podiatrist.
ALF stands for 'Advanced Lightwire Functionals'.
- It is a method to align teeth and improve the bite without braces (orthodontic treatment).
- It addresses alignment of the bones (orthopedic treatment) using principles of cranial osteopathy.
- It brings about changes in muscle function to achieve stable results.
- ALF is a whole-body-and-mind approach to improve overall health and performance in every realm.
The STRENGTHS of ALF are
- cosmetics - barely visible from the outside
- gentle - far less discomfort than with braces
- stable - no need for life-long retention